Since 2005, I have in my spare time, been working on a project that I was invited to join by a start up company called Neotract Inc which is based in the Bay area of San Francisco. The company was initially made up of a small group of engineers who had a great idea of how a minimally invasive device could be created to treat male lower urinary tract symptoms (LUTS). Over the years, minimally invasive devices to treat LUTS as a consequence of benign prostatic hyperplasia involved destroying prostate tissue whether it be by freezing, cooking, steaming, lasering or even microwaving. Whilst less invasive than procedures that physically removed prostate tissue at the time of surgery, these still required a period of recovery and there was often a delay in deriving full benefit due to the need for tissues to recover after destructive energy or one sort or another had been applied to the prostate. The idea was to use a mechanical implant that would pull open the prostate urethra.
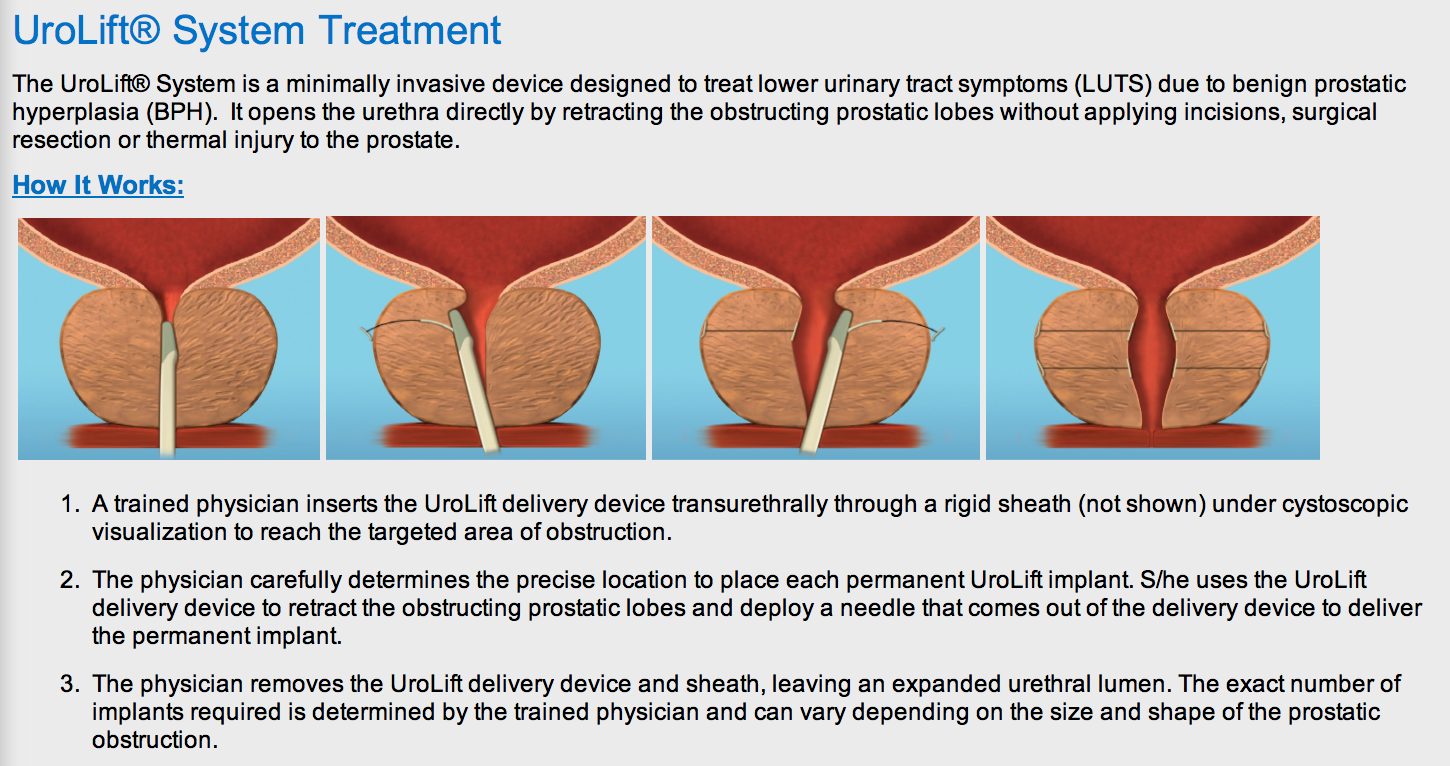
(Screenshot taken from www.neotract.com)
Through my involvement with Neotract, I was able to provide clinical input as well as being part of the clinical trials. This has lead to a number of publications that can easily be found by searching under my name and the search term either prostate or urolift. This month, we have seen this technology finally achieved US FDA approval. I wrote a piece about the benefits of clinicians and engineers working together for the BJUI Blogs. I was deeply moved to receive the following letter from Josh Makower, Chair of the Board of Neotract, Inc. I felt compelled to share this letter (with permission) which was addressed to myself and my co-investigator Dr Peter Chin.
Dear Henry and Peter –
This morning I opened my email and found this... http://www.bjuinternational.com/bjui-blog/urolift-takes-off-from-down-under-the-potential-rewards-when-engineers-bring-you-into-their-inner-circle/
I must say, Henry’s words brought a small tear to my eye. After 9 years of amazing struggle against many obstacles, our small team of passionate dedicated people have finally made it through a most significant hurdle towards bringing this technology to patients in the US. It’s a milestone that for many years seemed almost un-attainable and there were many dark days,.. but perseverance, trust and a vision held us together.
Henry and Peter – you were the first. There are always those who go first and history thankfully will mark them as innovators and leaders. You went where no one had gone before and gave us your time, your ideas and your talent towards a dream. That dream is one step closer to being realized and we would not be here if it were not for the two of you. When procedures and technologies become mainstream medicine, people often forget what it took to get there. They forget, or do not even know, how much a toll such a process takes on our relationships as we invest our lives in bringing something like this to fruition. But for those of us who were all in the trenches together; for those of us who hunkered down, re-grouped, re-engaged, re-energized and stood up again to regain ground when all appeared lost, we will never forget you and never forget the team that brought us here.
On behalf of all us, Henry and Peter, thank you for your leadership and your partnership. Henry – you articulated something special that must be shared – the partnership between engineers, entrepreneurs and physicians needed to advance medical technology is an essential one that we must never lose. Without it, medical innovation would not happen. Thank you for sharing your thoughts and putting them to paper in such a special way. I hope thoughts like these help preserve that special balance of talents, interests and shared goals that truly have the power to change the world and make it a better place.
From all of us at ExploraMed and NeoTract, and for all the patients who will benefit from all our collective efforts – thank you.
Sincerely -
Josh